Mitigating the risks of skin pressure points in surgery.

As a senior at Tulane University, as most engineering students do, my Biomedical Engineering class split up into teams to do a senior project. Tulane’s Biomedical Engineering department has a tradition of bringing in members of the New Orleans community to introduce medical issues for which teams would design and engineer solutions, for example Team Gleason.
My team of five was most interested in the issue presented by Dr. Korndorffer, at the time vice chair of surgery at Tulane University Health Sciences Center. He discussed how patient positioning during extended surgical procedures can inadvertently cause pressure ulcers to form at pressure points on the skin, for example at bony protrusions or against devices for positioning the body during surgery.
These pressure injuries happen due to the pressure blocking the flow of blood in the capillaries of the skin. The lack of oxygenation directly damages the tissue, and restoring blood flow after that happens injures the tissue further, which is called a “reperfusion injury” and causes the ulceration of the skin.
Normally, people don’t get pressure ulcers from, for example, sitting in chairs or resting their elbows on a table, because they can consciously or subconsciously shift their body. These small movements allow blood to flow in the pressure point again without issue.
When you're under anesthesia, obviously you won’t be doing much moving. Therefore in surgery, staff have to ensure adequate padding of the pressure points, and sometimes will adjust the patient based on how long they’ve been in a given position. These preventative procedures can help, but pressure injuries can still happen on certain points, especially to older patients undergoing involved orthopedic procedures.
Ultimately, surgical staff have no visibility on the real issue: the actual pressures present on the skin at these points.
After brainstorming, we decided the best approach to the problem would be to provide a way to actually quantify the pressure at known sensitive locations on the body during surgery.
Pressure-sensing pads that visualize and quantify pressures across an area are a thing that existed, but none of the these solutions could stay in place on a specified location on a patient’s skin - a requirement if monitoring is to happen when a pressure point is obscured, or to be able to keep monitoring the point after a position adjustment.
So, we decided that we needed to design a pressure sensing pad that could adhere to a patient like a bandage, but still reliably provide real data about the pressures on the skin at its location.
Our research informed us that pressure sensing pads use a matrix of cells of material that change resistivity when compressed. So, the design challenge became to find materials that would work for the pressure sensitive cells, physically separate them, and electrically connect them into a matrix, all of which would have to be flexible and soft against a patient’s skin.
We investigated options for materials together, and tried several in matrices. I did a portion of the assembly, and managed all the electronics and programming using an Arduino to poll the arrays of pressure cells. This way, I found that using conducting foam gave the best responses to pressure, connected by conductive fabric strips and separated into cells with insulative open-cell foam. I was able to verify this result by testing the foam directly with an Instron in compression.
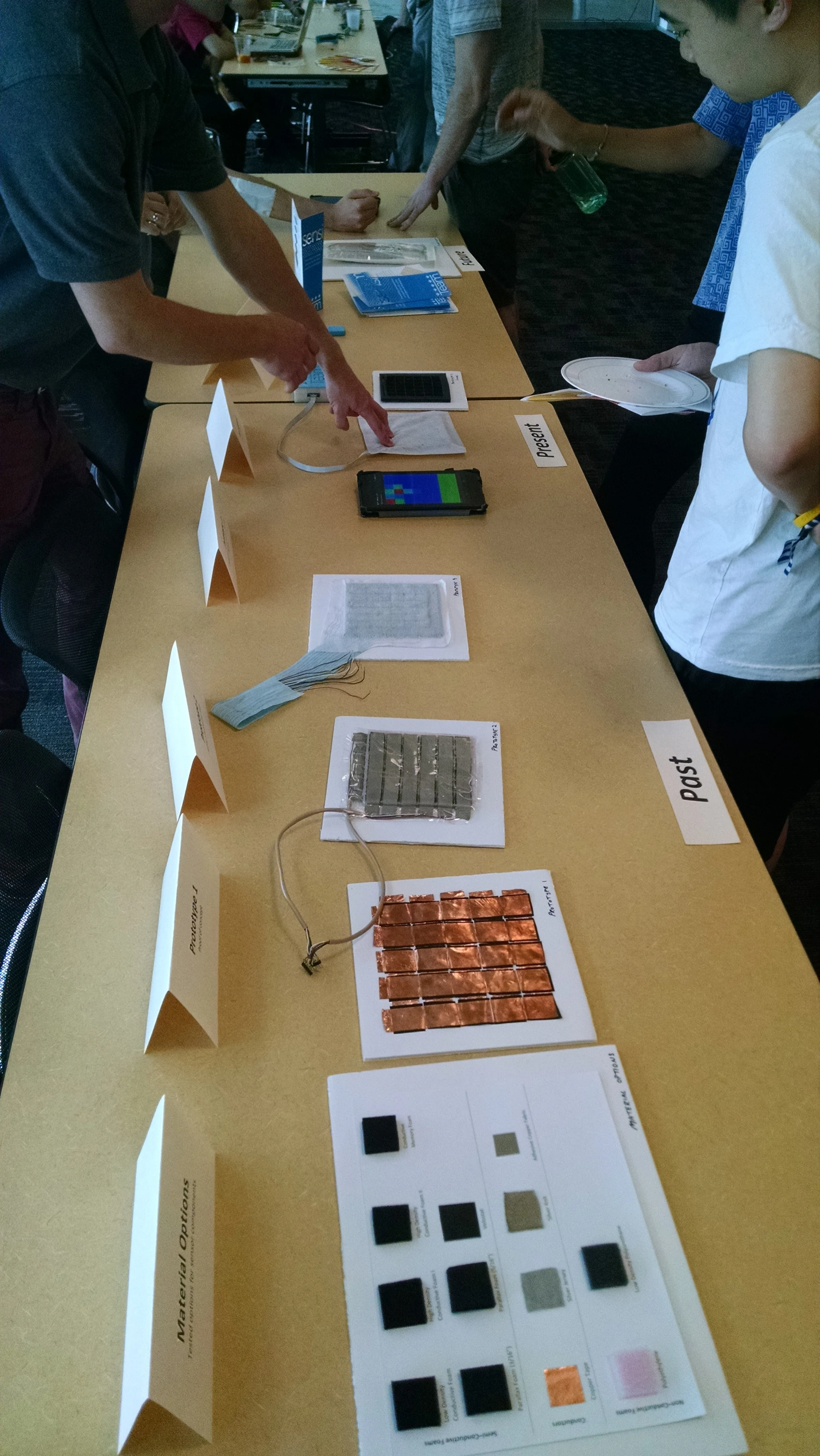
Our table setup at the senior design show. At the bottom are several options for materials we investigated. Progressing towards the top, you can see the iterations of patch prototypes.
We wanted the patch system to work wirelessly, so to show this was feasible, I had to migrate the system from from a patch wired to an Arduino, connected to a laptop, and programmed with C++ in the Arduino IDE, to something with Bluetooth Low-Energy (BTLE) capability. This meant that I had to re-implement the embedded code to poll the array of cells and send the data for the nRF52 microcontroller, which at the time was not supported in the Arduino IDE or CircuitPython, which meant I had to program it in C.
We also needed something to receive the pressure data coming off the patch and to visualize it, as well as represent the relative risk of the pressures over time. For this, I developed an Android application in Java to do exactly that.
We could tell we had something unique with our bandage-like sensor, and so we filed a provisional patent application for the technology. At the senior design show not long after, our design and prototypes were very well reviewed, and we received second place in the show! This reinforced our belief that we had a concept worth attempting to commercialize.
We founded Nisoltus Medical, LLC to do exactly that, and began to search for sources of funding. I had taken a course in entrepreneurship offered by the Biomedical Engineering department, and so was well-equipped to use tools such as the Business Model Canvas to plot a course to revenue for us to pursue, while reaching out to suppliers to model the production costs of our technology and possible profits, and collecting information about the certifications necessary to ensure our product could be used as we intended.
Our team, now as a corporate entity, received mentorship from a number of sources. We met with orthopedic surgeons from the Tulane School of medicine to get feedback on our design, to see how we could iterate the design and alerting methodology to best fit their workflows in the operating suite. We also utilized the close ties Tulane has with the New Orleans BioInnovation Center to iterate our business planning, and to identify sources of preliminary funding.
We submitted our plans to several grant competitions, and won first place and $25K from the 2016 Tulane Business Model Competition, $5K from the International Business Model Competition, and $5K from VentureWell’s E-Team program. The last of these was contingent on attending a three-day business development workshop in Cambridge, MA, which I did with one of my teammates, further improving our plans, especially in value chain analysis to understand the upstream elements on which our technology was dependent, and its downstream effects on that of surgeries and surgical outcomes.
Unfortunately, after our initial successes in the grant competitions, we were unable to gain much more attention or interest in our technology. Even though we had funding that we could use to further improve our prototypes, it wasn’t enough to produce them en masse, or for any of us to be able to work on work on the project full-time.
If I were to hazard a guess, healthcare systems became more aware of the potentiality of pressure-related injuries from surgical procedures, and so improved existing padding and shifting procedures in surgery, which would not implicate the purchase of additional products for procedures that may not be able to have their billing adjusted to compensate.
We closed Nisoltus Medical, LLC a little over four years after we first started working on the problem of pressure-related injuries from surgical procedures. Despite ending with a fizzle, I am really happy to have had the entrepreneurial experience of developing a technology, business planning to bring it to market, and successfully securing some funding.

Special thanks to my teammates Leah Gerber, Scott Stewart, Chris Sloas, and Conor Vickers!